
Abstract
The National Health Expenditure Accounts (NHEA) produced by the Centers for Medicare and Medicaid Services report that U.S. health care spending was $2.6 trillion in 2010. More recent estimates from Altarum Institute confirm that the health sector represents 17.9 percent of our national output. The data from the Bureau of Labor Statistics show that the health sector continued to create jobs throughout the recession and recovery and now accounts for nearly one in nine jobs. For the first time, we link the workforce by occupation to national spending on health care services by aligning data sets from the BLS and Bureau of Economic Analysis with the NHEA. We find $1 trillion, or 57 percent of the $1.78 trillion spent on personal health care services, went to health sector labor. Characterizing the health sector workforce and its contribution to health expenditures informs the potential for spending reductions and the implications of such reductions on employment.










Similar content being viewed by others

Notes
There is evidence that the spending growth slowdown began in 2005, thus pre-dating the Great Recession [Kaufman 2012; Roehrig and others 2012].
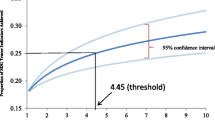
For longer historical context, the health share of total employment was 4.4 percent in 1970 and 5.9 percent in 1980. Also, health care absorbed 7.2 percent of GDP in 1970 and 9.1 percent of GDP in 1980.
Even with the aforementioned slowdown in health care expenditure growth, concerns over spending sustainability are legitimate [Roehrig 2012].
Note that there is a considerable lag between release of the once every 5-year “benchmark” input-output table and the reference year. For example, the 2007 benchmark input-output data will not be released until the end of 2013. This means that analysts must use the annual input-output tables which are dramatically less detailed and subject to revisions, as economic census data that lie behind the benchmark tables are interpolated and extrapolated, while waiting for the next release.
OACT was going to have the University of MD INFORUM model (Inter-industry Forecasting Project)—a dynamic input-output model embedded in a macro model—project occupations within industries, but this plan was never executed [Freeland 2012].
Compensation=0.7Compensation × Benefits Inflation Factor=>Benefits Inflation Factor=1/0.7=1.4.
Conversely, there are significant numbers of individuals in health occupations that work outside of health industries, notably pharmacists who work in the retail sector or instructors who work in educational settings.
The American Recovery and Reinvestment Act (ARRA) of 2009, under its Health Information Technology for Economic and Clinical Health (HITECH) provision, aims to move the nation toward a paper-less health information network via the widespread adoption of electronic health records.
References
Altarum Institute. 2012. Health Sector Economic Indicators Spending Brief #12-11, September 2012 Data, Altarum Institute, November 8, 2012. http://www.altarum.org/files/imce/CSHS-Spending-Brief_Nov_percent202012.pdf.
Baicker, Katherine, Amitabh Chandra, and Jonathan Skinner . 2012. “Saving Money or Just Saving Lives? Improving the Productivity of US Health Care Spending.” Annual Review of Economics, 4 (July): 33–56.
Freeland, Mark. 2012. Personal communication with author, June 26
Institute of Medicine (IOM ). 2012. Best care at lower cost: The path to continuously learning health care in America. edited by Mark Smith, Robert Saunders, Leigh Stuckhardt, J. Michael McGinnis, eds. Washington, DC: The National Academies Press.
Kaiser Family Foundation. 2012. Health Care Costs: A Primer—Key Information on Health Care Costs and Their Impact, May. http://www.kff.org/insurance/upload/7670-03.pdf.
Kaufman, Ken . 2012. Bending the Health Care Cost Curve: More Than Meets the Eye? Health Affairs Blog, April 13. http://healthaffairs.org/blog/2012/04/13/bending-the-health-care-cost-curve-more-than-meets-the-eye/.
Kim, D., T. Gilmore, and W. Jolliff . 2012. “Annual Industry Accounts: Advance Statistics on GDP by Industry for 2011.” Survey of Current Business, 92 (5): 6–22.
PwC, 2012. Medical Cost Trend: Behind the Numbers 2013, PwC Health Research Institute, May. http://www.pwc.com/us/en/health-industries/behind-the-numbers/index.html.
Roehrig, Charles . 2011. The Case for Tracking Health Spending as a Share of ‘Potential’ GDP, Health Policy Forum, Altarum Institute, May 11. http://www.healthpolicyforum.org/post/case-tracking-health-spending-share-potential-gdp.
Roehrig, Charles . 2012. A New Look at the Simpson-Bowles Budget Plan: Implications for Sustainable Health Spending, Health Policy Forum, Altarum Institute, October 30. http://www.altarum.org/forum/post/new-look-simpson-bowles-budget-plan-implications-sustainable-health-spending.
Roehrig, Charles, Ani Turner, Paul Hughes-Cromwick, and George Miller . 2012. “When the Cost Curve Bent—Pre-Recession Moderation in Health Care Spending.” New England Journal of Medicine, 367 (7): 590–592.
Sing, Merrile, Jessica Banthin, Thomas Selden, Cathy Cowan, and Sean Keehan . 2006. “Reconciling Medical Expenditure Estimates from the MEPS and NHEA, 2002.” Health Care Financing Review, 28 (1): 25–40.
Steuerle, Gene . 2009. “The New Spending Numbers: What They Tell Us, And What They Don’t,” Health Affairs Web Exclusive (February 24).
Acknowledgements
The authors would like to thank Tamara Crouter for providing data analysis and programming support to this effort and Dr. Charles Roehrig, Director of Altarum's Center for Sustainable Health Spending, for originating the project concept and providing technical assistance and review. We would also like to thank three anonymous reviewers for helpful comments.
Additional information
This paper was a winner of the NABE Contributed Paper Award for 2012 and was presented at the NABE Annual Meeting in October 2012.
*Ani Turner is a Senior Health Policy Analyst and Deputy Director of the Altarum Institute Center for Sustainable Health Spending. In addition to her research management role, she leads the Center's health workforce analysis and modeling and monthly tracking of health sector employment. As a consultant to government and commercial clients for over two decades, she has developed models and conducted analyses of health-care resources, costs, and quality for the Department of Health and Human Services, the Department of Defense, individual States, and private health plans. She received her BA in Mathematics, summa cum laude, Phi Beta Kappa from the University of Michigan, where she is currently completing the Master of Applied Economics program. Paul Hughes-Cromwick, MA, is Senior Health Economist, Center for Sustainable Health Spending, Altarum Institute, based in Ann Arbor, Michigan, where he leads outreach and business development. Prior to Altarum, he worked at the University of Michigan School of Nursing; the Henry Ford Health System; the University of Pittsburgh Graduate School of Public Health; the State of Connecticut, where he was Research Director for the Connecticut Partnership for Long Term Care Insurance; and the U.S. Department of Health and Human Services Office of the Assistant Secretary for Planning and Evaluation. Mr. Hughes-Cromwick serves on the Board of Health Alliance Plan HMO in Detroit, and chairs the NABE Health Economics Roundtable. He has a BS in math and philosophy from the University of Notre Dame and an MA in applied economics from Clark University, Worcester, Massachusetts.
Rights and permissions
About this article
Cite this article
Turner, A., Hughes-Cromwick, P. Connecting U.S. Health Expenditures with the Health Sector Workforce. Bus Econ 48, 42–57 (2013). https://doi.org/10.1057/be.2012.35
Published:
Issue Date:
DOI: https://doi.org/10.1057/be.2012.35