
Abstract
This article deals with repurposing of the epidermal growth factor (EGF) to the treatment of diabetic foot ulcers (DFU) grades III and IV, according to the Wagner scale. The design of a repurposing commercial strategy is described in this document as a contribution to a body of knowledge with high uncertainty and lack of methodology for decision-makers. An analysis of the potential market suggested a significant impact of the product Heberprot-P® on costs associated to DFU treatment. Unexpected findings, obtained from a study of the competence, are reported here. The feasibility of a repurposing strategy containing short-, medium- and long-term action plans, without mutual interferences, and adopting strategic intent, strategic assessment and strategic choice as fundamental concepts is demonstrated in this work.
Similar content being viewed by others


INTRODUCTION
A business strategy often called ‘drug re-profiling’ (repurposing) allows market re-positioning by finding a new medical application for a known molecule.1, 2 Repurposing strategy reduces commercial risks, since candidate molecules have overcame initial pre-clinical and clinical phases, and as a result safety and pharmacokinetic profiles are well-known. Shorter routes to regulatory approval may be found, because in vitro and in vivo assays, chemical optimization, toxicology and technology development often can be avoided. Important regulatory challenges may shadow the low-risk profile of a repurposing strategy: (i) new end points and efficacy measures should be created,3, 4, 5 (ii) clinical data to validate the action pathways may be unavailable, limited to previous indications or unacceptable because regulations have changed and (iii) overlapping of previous and new indications may be unavoidable during development phases.6
More than 15 years of repurposing activity in the pharmaceutical industry suggest persistence of new medical indications, because no drug has been fully understood. Evidences of potential repurposing arise from medical observations, as in the Sildenafil case,7 innovative information (for example Duloxetine repurposing),8 or from technology platforms implemented for identifying commercial opportunities.9 Applications of science at CIGB have been supported by basic research, and discovery activity has been driven by researchers’ interest in gaining a deeper understanding of diseases, and finding useful medicines and treatments.10 One of such medicines (Heberprot-P®), containing epidermal growth factor (EGF) as the active pharmaceutical ingredient (APhI), was developed to treat advanced diabetic foot ulcers (DFU), which is the most common cause of non-traumatic lower extremity amputations in the industrialized countries, let alone in developing countries. Here we report components, dynamics and challenges of EGF's repurposing for solving an urgent unmet medical need.
METHODOLOGY
Repurposing management
A new medical indication was identified by the CIGB's research staff in experiments with EGF in animal models. Promising experimental results were followed by market and clinical studies, intellectual property claims, and strategy planning. Potential usefulness of EGF as APh I of a parentheral product (Heberprot-P®, Heber Biotec, Havana) was evaluated, and the indication scope was defined. The first units of Heberprot-P® were manufactured in a pilot-plant under clean room conditions at CIGB, Havana, Cuba;11 additional manufacturing facilities were built in Europe; and the first clinical study was performed after finding a market niche with the highest success opportunity. Clinical results allowed for the design of a regulatory route to obtain approval for commercialization of Heberprot-P®, and a global penetration strategy in the pharmaceutical market. Regulatory route was shifted from ‘orphan drug’ to ‘full registration’ according to recommendation of the European Medicine Agency (EMEA). The commercial strategy included short-, medium- and long-term action plans that were performed in parallel, avoiding noxious mutual interferences.
Total management
Research, pharmaceutical development, pre-clinical and clinical studies, regulatory and intellectual property issues, manufacturing, negotiations, and commercial tasks were coordinated by the ‘Heberprot-P® task force’, following the total management principle. Coordination was performed by the Product Management Team, directly subordinated to the General Direction with constant intensive interventions of all institutional directions (research, development, regulatory affairs, etc.).
Strategic design
Strategic intent started from product national extension, followed by introduction in the current market positions of Heber Biotec S.A., and simultaneously reaching the developed countries market. Strategic assessment was performed to determine medical indication scope, market niche dimension and competitors’ strength. Strategic choice included actions, finding strategic alliances to accelerate development, and penetration of Heberprot-P® in the most demanding markets.
Master plan
A document containing fundamental strategic components to develop and commercialize Heberprot-P® was elaborated as a master plan. Negotiation and commercialization intents were described in the master plan, as well as intellectual property issues, regulatory challenges, manufacturing requirements, status of pre-clinical, non-clinical and clinical studies, future developments, approvals for commercialization, novel medical indications, pharmaceutical formulations, tactic and strategic weakness, critical issues, action plans, and solutions to weakness and critical issues. The master plan is dynamically updated, according to strategy advances, new data and useful experiences.
STARTING POINT
EGF was identified and characterized by the Nobel Prize Stanley Cohen, 40 years ago.12 Dr Cohen injected extracts of salivary glands in new-born mice, and observed an unprecedented maturation of epithelial structures. Later, he identified EGF and characterized its biological activity: (i) to stimulate and regulate cell proliferation, (ii) to promote cell migration and (iii) to favour cell and tissue differentiation, participating in the morphogenesis of epithelial organs. For the first time, scientists obtained a factor that stimulated epithelial cell growth and maturation that allowed investigating such growth.
Many studies have shown EGF to be a potent stimulating growth factor for a variety of cell lines.13 The protection activity of EGF against CCl4-induced hepatic injury has been demonstrated in experiments with female Sprague-Dawley rats.14 A multi-organ failure induced by thioacetamide was attenuated with single EGF prophylactic intervention, preventing damages in kidney, liver and intestine, simultaneously.15 The effect of a single EGF systemic intervention in mice and rats, 30 min before thermal injury, was examined. Reduction of intestinal necrosis and renal hemorraghic foci, jejunum protection, and attenuation of lung damages were observed in these experiments.16 Acute ischemia/reperfusion injury, inducing multi-organ failure was reproduced in a more clinically relevant rat model. Pre-treatment with EGF truncated intestinal damages, neutrophilic infiltration and lipid peroxidation. Lung and renal injuries induced by ischemia/reperfusion were also reduced.17 More research was performed to obtain a deeper understanding of the EGF citoprotection activity,18, 19, 20 before starting clinical studies in DFU patients.
Healing time of DFU is usually in the range between 29 and 52 weeks, depending on the lesion complexity.21 Tissue granulation was significantly different from that commonly observed in patients with complex ulcers in clinical studies with EFG infiltration.22, 23 Lower limbs were saved from amputation in 58–60 per cent of patients, and ulcer granulation was observed after 2 weeks in 78 per cent of patients (Figure 1). Granulation tissue stimulation observed during phase III clinical trial was highly predictive of wound closure, because two dose levels fulfilled the >30 per cent threshold advantage over the control group for the 2 weeks main outcome.24 This finding could be useful as a decision point to identify non responders that would require other medical strategies. Results of clinical trials with Heberprot-P® have deep implications for current clinical practices, have given rise to actual hopes for patients, because this treatment offers additional surgical alternatives to medical doctors, and have suggested that treatment contributes to reduce amputation rates to an unexpected low level. Enough scientific evidence has qualified the EGF as a first line therapeutic intervention that may be reserved for life-threatening conditions or disabling processes.25

Correlation between granulation response and complete healing during follow-up.
MARKET NICHE
The treatment of advance diabetic wounds is an unexplored market niche, because there is no medical solution for grades III and IV ulcers, and amputation is the treatment generally recognized by medical consensus as standard procedure.26 Costs of diabetes-related foot ulcers and amputations in Europe have been estimated to be 10 billion Euros per year. Estimates of DFU treatment costs were between 2452 and 79 495 USD/patient, according to reports published between 1994 and 2000 in Sweden, USA, Belgium, UK and Switzerland. Recent direct cost measurements, as a function of disease severity, were in the range of 5756–21 469 USD/patient. Measurements associated to outcomes showed that costs of DFU treatment were higher than 9800 USD/patient if ulcer heal, 11 035 USD/patient if unhealed, and 32 165 USD/patient if DFU advances to major amputation.27, 28 Single-centre studies have also demonstrated that the economic impact of DFU is significantly high.29, 30, 31, 32 Current costs of advanced wound treatments have not been reported in the literature.
Ulcer infection risk was significantly reduced as healing time of recalcitrant foot ulcers diminished during phase I–III clinical trials, and national extension of Heberprot-P®. Consequently, costs associated to ulcer infection (17 000 USD/patient), and debridement (5064–7104 USD) were also reduced. In addition, amputation risk was also reduced, because 66 per cent of patients were rescued from amputation in clinical trials, and 82 per cent during national extension phase, avoiding associated costs. Care costs of chronic wounds are assumed to increase as wound severity, as well as with the presence of complications (cellulitis or osteomyelitis). Care ulcers not complicated by infection cost 775.55 USD/month, compared to the 2048.52 USD/month for ulcers complicated with cellulitis, and 3 798.27 USD/month for ulcers complicated with osteomyellitis.29
REPURPOSING STRATEGY
Designing a commercial strategy is a non-lineal process that involves forecasting, and finding advantages.33 Small changes in a qualitative or quantitative variable give rise to inflexion points that require radical changes, even in the most carefully planned strategy.34 Consequently, there is not an absolute method to design a commercial strategy, but three logical components have been identified in study cases: (i) strategic intent, (ii) strategic assessment, and (iii) strategic choice.35 This body of knowledge was taken as fundamental for designing a repurposing strategy to introduce Heberprot-P® in the pharmaceutical market.
The strategic intent was almost immediately evident from a study of products available in the market. Study findings were the following:
-
1
Amputation is the unique alternative for DFU grades III and IV, according to Wagner's scale.36
-
2
There is not investigational new drugs (IND) intended for advanced DFU waiting for regulatory approval.
-
3
There have not been new drug applications (NDA) approved for DFU treatment since 2001.
-
4
There is not perceptible competence between big pharmaceutical companies as usual in cancer, HIV, cardiovascular and other attractive medical fields.
-
5
Available products have shown low efficacy, and reproducibility for small ulcers (grades I and II).
-
6
Clinical data suggest little advances in the study of DFU.
-
7
Current products for DFU treatment have shown higher probability to be non-effective than the contrary.
-
8
Poor scope of medicines indicated for this disease leaves a narrow margin of success to medical doctors.
-
9
More than 10 weeks are necessary to observe clinical differences if current products are used.
-
10
A time window of 20 weeks, suggests poor satisfaction.
-
11
Granulation and epithelization have not been characterized as separate process in studies with current products.
-
12
Recurrences are abundant.
-
13
Protease action on wound area is a serious limitation.
-
14
Products and treatments are highly expensive.
-
15
Excessive heterogeneity is observed in clinical results with different products.
-
16
Assuming that healing probability of current products would increase 2-fold, ¿what will be the best alternative for refractory patients?
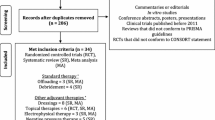
These findings suggested the business strategy direction as globally oriented, because the market niche was identified as unique. The CIGB's commercial strategy involves expanding sales into new markets, while maintaining current established positions, promoting early-stage associations for joint development of projects, and sharing opportunities with partners.37 A second direction strengthened the strategy low-risk profile: the national extension of Heberprot-P®. Identifying this branching off on the strategic intent was not a difficult task, because the Havana Scientific Pole has been coordinating multi-institutional approaches, and introducing scientific results into the Cuban health system for 20 years.10 The external context and internal capacities were evaluated to perform the strategic assessment.38 Global orientation was not affected by simultaneous implementation of short-, medium- and long-term action plans. A deeper study of the competence revealed an attractive commercial opportunity (Figure 2), and costs of DFU treatments reinforced this perception ( Table 1).

Comparison of Heberprot-P® with products available in the pharmaceutical market.
The strategic choice included an assessment of the medical indication scope as regard to attainable market niche, epidemiology statistics, intellectual property, competitive environment, alternative clinical development routes and negotiation strategies. First, a patent claiming the invention of a pharmaceutical composition and an application method was granted in the United States, Cuba, México, South Africa, Europe, Russia, Ukraine, China, South Korea, Hong Kong, India, Singapore and Australia.
A repurposing generates a significant value of intellectual property, but since EGF is well known by the scientific community, risk that previous knowledge annulate patent claims was persistent in every strategy analysis. Researcher's scepticism was a serious challenge, because EGF had never been tested for DFU treatment in other scientific institutions. The novelty of the pharmaceutical composition and application method of a product intended for an urgent unmet medical need built the intellectual property of Heberprot-P®.
Second, commercialization agreements with seven foreign companies were signed, after regulatory approval in each country. Negotiations have been started with companies from Algeria, Argentina, China, Russia, Colombia, Brazil, Mexico, Azerbaijan, Turkey, USA, France and South Africa. Third, the product was introduced in the current market positions of Heber Biotec S.A., which allowed obtaining additional clinical experience, credibility, significant incomes from sales and intangible assets, and opening negotiation alternatives. After approval for commercialization, 4000 patients have received benefits in Cuba, 4400 in Venezuela and 200 in Algeria. Recently, application of Heberprot-P® has been started in Argentina, Uruguay and Dominican Republic.
Medium- and long-term action plans included finding corporate partnership for out-licensing to selected territories (North America, Japan and Australia). (http://heberprot-p.cigb.edu.cu, http://gndp.cigb.edu.cu/index.html) The European Medicines Agency (EMEA) recommended abandoning the application as ‘orphan drug’, after evaluating clinical evidences, because Heberprot-P® may reach a broader disease niche. Certainly, it could not be argued that the product were not effective in DFU grades I and II. The support of European regulatory advisory companies was a very valuable component of the strategy to change the application to ‘full registration’: (i) new action plans were designed and implemented, (ii) new clinical trials were necessary, (iii) documents were prepared according to European requirements, and (iv) corrective actions on manufacturing facilities and technology transfer operations were performed.
CONCLUSIONS
The feasibility of designing and performing a strategic plan for repurposing the EGF to solve an unmet medical need was the hypothesis tested in this work. The product Heberprot-P® was approved for commercialization, and introduced in the Cuban health system for treatment of DFU patients, as part of a short-term action plan. Regulatory approvals and commercial agreements were obtained in a second phase of the strategy, and the product was introduced in traditional Heber Biotec's markets. The scope of the proposed medical indication was defined, and the commercial strategy was global with a unique market niche. A long-term action plan to introduce Heberprot-P® in high price markets will certainly change the cost–benefit ratio in favour of DFU patients. Short-, medium-, and long-term action plans were performed in parallel, without mutual interferences, nor affecting the global strategy. Strategic alliances were signed, and the product was submitted for approval to the European regulatory agency as ‘full registration’, because the market niche was broader than expected.
References
Longman, R. (2004) Pharmaceutical strategies: Jumpstart to products. In Vivo 22: 17.
Stuart, M. (2004) Re-discovering existing drugs. Start-Up 9: 23–30.
Rosen, R.C., Riley, A., Wagner, G., Osterloh, I.H., Kirkpatrick, J. and Mishra, A. (1997) The international index of erectile function (IIEF): A multidimensional scale for assessment of erectile dysfunction. Urology 49 (6): 822–830.
Thor, K.B. (2001) Methods of using rapid-onset selective serotonin reuptake inhibitors for treating sexual dysfunction. World Intellectual Property Organization Patent 01/17521: A1.
Norton, P.A., Zinner, N.R., Yalcin, I., Bump, R.C. and Duloxetine Urinary Incontinence Study Group. (2002) Duloxetine vs. placebo in the treatment of stress urinary incontinence. American Journal of Obstetrics Gynecol 187 (1): 40–48.
Cowen, S.G. (2003) Pharmaceutical Industry Pulse. New and generic drug approvals: 1998–2004. Centre for Drug Evaluation and Research. CDER Reports to the Nation, October, http://www.fda.gov/downloads/AboutFDA/CentersOffices/CDER/WhatWeDo/UCM078941.pdf.
Kolata, G. (1998) US approves sale of impotence pill; huge market seen. The New York Times A1.
Thor, K.B. and Katofiasc, M.A. (1995) Effects of duloxetine, a combined serotonin and norepinephrine reuptake inhibitor, on central neural control of lower urinary tract function in the chloralose-anesthetized female cat. The Journal of Pharmacology and Experimental Therapeutics 274 (2): 1014–1024.
Ostrov, B.F. (2004) Renewed life for old drugs. San Jose Mercury News, 1E.
Mola, E.L., Silva, R., Acevedo, B., Buxadó, J.A., Aguilera, A. and Herrera, L. (2007) Taking stock of Cuban biotech. Nature Biotechnology 25 (11): 1215–1216.
Montané, M.E. et al (2009) Performance evaluation of a pilot-plant for investigational new drugs. The Journal of Agriculture, Biotechnology and Ecology 2 (2): 189–204.
Cohen, S. (1962) Isolation of a mouse submaxillary gland protein accelerating incisor eruption and eyelid opening in the new-born animal. The Journal of Biological Chemistry 237 (5): 1555–1562.
Playford, R.J. et al (1995) Epidermal growth factor is digested to smaller, less active forms in acidic gastric juice. Gastroenterology 108 (1): 92–101.
Berlanga, J. et al (1998) Epidermal growth factor protects against carbon tetrachloride-induced hepatic injury. Clinical Science 94 (3): 219–223.
Caballero, M.E. et al (2001) Epidermal growth factor reduces multiorgan failure induced by thioacetamide. Gut 48: 34–40.
Berlanga, J., Lodos, J. and López-Saura, P. (2002) Attenuation of internal organ damages by exogenously administered epidermal growth factor (EGF) in burned rodents. Burns 28 (5): 435–442.
Berlanga, J. et al (2002) Prophylactic use of epidermal growth factor reduces ischemia/reperfusion intestinal damage. American Journal of Pathology 161: 373–379.
Berlanga-Acosta, J., Playford, R.J., Mandir, N. and Goodlad, R.A. (2001) Gastrointestinal cell proliferation and crypt fission are separate but complementary means of increasing tissue mass following infusion of epidermal growth factor in rats. Gut 148: 803–807.
Sasaki, M., FitzGerald, A.J., Mandir, N., Berlanga-Acosta, J. and Goodlad, R.A. (2003) Keratinocyte growth factor and epidermal growth factor can reverse the intestinal atrophy associated with elemental diets in mice. Experimental Physiology 88: 261–267.
Cibrián, D. et al (2006) Use of growth-hormone-releasing peptide-6 (GHRP-6) for the prevention of multiple organ failure. Clinical Science 110: 563–573.
Tennvall, G., Apelqvist, J. and Eneroth, M. (2000) Costs of deep foot infections in patients with Diabetes mellitus. PharmacoEconomics 18 (3): 225–238.
Berlanga, J. et al (2006) Epidermal growth factor intra-lesional infiltrations can prevent amputation in diabetic patients with advanced foot ulcers. International Wound Journal 3 (3): 232–239.
Fernández-Montequín, J.I. et al (2007) Intra-lesional injections of Citoprot-P® (recombinant human Epidermal Growth Factor) in advanced diabetic foot ulcers with risk of amputation. International Wound Journal 4 (4): 333–343.
Fernández-Montequín, J.I. et al (2009) Intra-lesional injections of recombinant human epidermal growth factor promote granulation and healing in advanced diabetic foot ulcers: Multicenter, randomized, placebo-controlled, double-blind study. International Wound Journal 6 (6): 432–443.
Berlanga-Acosta, J. et al (2009) Epidermal growth factor in clinical practice. A review of its biological action, clinical indications and safety implications. International Wound Journal 6 (5): 331–346.
Frykberg, R.G. et al (2000) Diabetic foot disorders. A clinical practice guideline. Journal of Foot and Ankel Surgery 39 (5 Sppl): S1–S60.
Prompers, L. et al (2008) Prediction of outcome in individuals with diabetic foot ulcers: Focus on the differences between individuals with and without peripheral arterial disease. The EURODIALE Study. Diabetologia 51: 747–755.
Prompers, L. et al (2008) Resource utilisation and costs associated with the treatment of diabetic foot ulcers. Prospective data from the Eurodiale Study. Diabetologia 51: 1826–1834.
Habacher, W. et al (2007) A model to analyse costs and benefit of intensified diabetic foot care in Austria. Journal of Evaluation in Clinical Practice 13(6): 906–912.
Girod, I., Valensi, P., Laforet, C., Moreau-Defarges, T., Guillon, P. and Baron, F. (2003) An economic evaluation of the cost of diabetic foot ulcers: Results of a retrospective study on 239 patients. Diabetes Metabolism 29: 269–277.
Smith, D., Cullen, M.J. and Nolan, J.J. (2004) The cost of managing diabetic foot ulceration in an Irish hospital. Irish Journal of Medical Sciences 173: 89–92.
Matricali, G.A., Dereymaeker, G., Muls, E., Flour, M. and Mathieu, C. (2007) Economic aspects of diabetic foot care in a multidisciplinary setting: A review. Diabetes Metabolism Research and Reviews 23: 339–347.
De Karen-Silver, M. (1997) Strategy in Crisis. London: Macmillan.
Grove, A.S. (1996) Only the Paranoid Survive: How to Exploit the Crisis Points that Challenge Every Company and Career. London: Harper Collins Business.
Campbell, A. (1999) Tailord, not benchmarked: A fresh look at corporate planning. Harvard Business Review March–April: 41–50.
Wagner, F.W. (1983) Algorithms of diabetic foot care. In: M.E. Levin, F.W. O’Neal (eds.) The Diabetic Foot. St Louis, MO: Mosby, pp. 290–295.
Mola, E.L., Silva, R., Acevedo, B., Buxadó, J.A., Aguilera, A. and Herrera, L. (2006) Biotechnology in Cuba: 20 years of scientific, social and economic progress. Journal of Commercial Biotechnology 13 (1): 1–11.
Drain, P. and Barry, M. (2010) Fifty years of US embargo. Cuba's health outcomes and lessons. Science 328 (April 30): 573.
Tennvall, G.R. and Apelqvist, J. (2005) Counting the costs of the diabetic foot. Diabetes Voice (Special Issue) 50: 8–10.
Author information
Authors and Affiliations
Corresponding author
Additional information
2works as Chemical Engineer in the Direction of Manufacture at the CIGB. Previously, he worked at the GNDP for 2 years. He has been working in the sector for more than 15 years.
Rights and permissions
About this article
Cite this article
Mola, E., Buxadó, J. & Herrera, L. Repurposing of the epidermal growth factor. J Commer Biotechnol 17, 45–52 (2011). https://doi.org/10.1057/jcb.2010.28
Received:
Revised:
Published:
Issue Date:
DOI: https://doi.org/10.1057/jcb.2010.28